
Issue One: A tipping point
Issue One: A tipping point
3.14.20 | An introduction to the new Coronavirus on the week it could no longer be ignored

Hello there.
First of all thank you—really, thank you—for signing up for this newsletter. On Thursday morning I was texting with some friends about the Coronavirus epidemic, as I’d been doing off and on for weeks. Something felt different that morning, though. The wave of closures that followed the WHO’s pandemic designation, the overlapping announcements of celebrities and government officials testing positive for the virus, the botched Oval Office address — it felt like we’d reached a tipping point.
I posted an Instagram* story asking if anyone thought it would be helpful for me to start a newsletter covering how I was tracking and thinking about the crisis. The size of the response blew me away, and judging from the volume of signups from emails I don’t recognize, what started as a kind of open notebook for friends has taken on a life of its own. Which is great! Welcome!
If you’ve been reading obsessively already about the pandemic, this first email might contain a bunch of information you’re already familiar with. But based on the questions I’ve been getting from people, I thought it was best to start with the fundamentals. I can respond individually to emailed questions and will do a roundup of answers starting next week.
As we go on from here, I’ll be grateful for your tips, questions, and constructive criticism. Hopefully I’ll learn as much from you as you learn from me, and we’ll all be better off because of it.
You can write me here: covodyssey@gmail.com.
* I appreciate those of you who have requested to follow me on the ‘gram after seeing a repost of my announcement. I keep my account locked down to a very tight circle, so please don’t be offended if I don’t accept.
In this issue:
Introduction: How we got here, and what you’ve signed up for.
Coronavirus basics including:
What is this virus?
How does it spread?
What are the symptoms?
How severe is it?
Isn’t this just like the flu?
How bad likely is it to get in the U.S.?
How long will this last?
Why does testing matter, and what went wrong with it?
What I’m watching for.
Further resources and what I couldn’t fit.

[Photo by Alfredy Falcone / LaPresse / AP]
// Introduction
I’ve been paying attention to the novel coronavirus outbreak since early January, when I read news reports of an unexplained new respiratory virus circulating in Wuhan. Pandemics had been on my mind for much longer. For my dissertation research I spent a lot of time talking to and observing the daily work of emergency managers, continuity planners, and other disaster risk management professionals in New York City. The threat of a global pandemic came up routinely as an area of concern, and it has long been a standing feature in planning documents and exercises. Since at least the 1980s, public health specialists have warned that new pathogens would spill over from animal hosts into humans and, since we would have little or no immunity, spread quickly across the population, carrying with it mass sickness and death. It’s not hypothetical, it has happened repeatedly: Ebola, HIV, SARS — even influenza, which hops between pigs, birds, and humans, in the process mutating in ways that are usually harmless but can occasionally give rise to a catastrophically dangerous new strain.
In other words, the pandemic we’re facing now is a long time coming. It’s been a landmark on our institutional futurescape, a column of smoke on the horizon that has sometimes seemed closer, sometimes farther away. Recent society-wide responses that might appear to be coming out of nowhere — the shutdowns and cancellations, the quarantines — are rooted in practical experiences earned through smaller-scale outbreaks, through the early stages of this outbreak, and a regular stream of planning, simulations, and exercises in governments, academia, corporate firms, and non-profits that well predates the present crisis.
For example: In 2018, the Center for Health Security at Johns Hopkins ran a meticulously detailed tabletop exercise enlisting current and former U.S. government officials to play out how the government would respond to a fast-spreading novel disease outbreak. Over the course of the day the players debated a lot of the same decisions we’re reading about in the news today: whether to close schools, what to do about troops stationed overseas, how to develop a vaccine and how to distribute it. By the end of the exercise, which spanned 20 months of in-game time, millions worldwide had died, the U.S. health care system had been nationalized, and the global economy had come to a halt. You can watch an archived livestream here (see also these smart write-ups from the New Yorker and Washington Post).
That same year, the World Health Organization released its priorities for disease research and prevention. At the bottom of the list it included “Disease X,” a placeholder representing a known unknown — the inevitability of a new pathogen entering human circulation and becoming a pandemic. According to one of the disease ecologists who helped coin the term, Covid-19 is the disease we should have known was coming.
But just because people have been expecting and planning for a pandemic like this doesn’t mean we’re ready for it. I wasn’t. By the end of January and into February, the more I read about the spread of the virus, especially paying attention to what scientists were saying, the more it seemed to fit the projections I had been reading about as planning assumptions.
I teach a class at Columbia, and once Covid cases began appearing in large numbers outside China I started preparing to move my teaching online. I wanted to move slowly and not freak out my students, so I introduced the idea gradually, and held a tele-seminar test with them the first week of March.
I told my students our test was just a precaution, and that I was looking forward to seeing them in person for our last class before spring break. That class never happened. That weekend my university hastily announced it was suspending classes and moving online-only, at first only through spring break, and then for the rest of the semester. It was an important lesson for me. You can plan and pay attention, and still get overwhelmed by the speed of events.
/ What you’ve signed up for
Here’s what this & future issues of the newsletter will contain:
Notes on (and links to) news articles and academic research I’m reading;
Questions I’m asking;
Things I’m looking for as signposts for the future;
Sources I’m using to stay informed;
What I’m doing to stay (relatively) healthy, sane and socially connected.
I’ll also answer reader questions to the best of my ability (write me at covodyssey@gmail.com). My plan is to send out a new edition every Saturday, with supplemental issues maybe to cover rapid developments.
I’m not going to offer health advice, will keep editorializing minimal and constructive, and will leave future projections to the specialists — epidemiologists, disease ecologists, and public health professionals. I’m also going to try to be disciplined in my epistemic humility. We’re still early in this pandemic, there is a lot we don’t know for certain, and some of what we think we know will turn out to be wrong.
To start out with everyone on the same page, I’ll begin with basics on the coronavirus itself.
// Coronavirus basics
What is this thing?
In shorthand we’re all talking about “The Coronavirus.” The scientific name for it is SARS-Cov-2 (Severe Acute Respiratory Syndrome-CoronaVirus-2). Coronavirus is the name of its viral family, four members of which are the germs that cause most cases of the common cold in humans. Other members of this viral family circulate among bats and birds and sometimes mammals.
It turns out bat coronaviruses spill over into the human population pretty often (here are two great NPR pieces on bat coronavirus spillovers and why bats can carry the virus without getting sick). Most of these spillovers are harmless. Some aren’t.
One spillover near Hong Kong in late 2002 sparked what we recognize now as the SARS outbreak which, before it was over in May of 2004, had infected 8,000 people and killed nearly 800. Another spillover event led to MERS (Middle-East Respiratory Virus), which scientists think moved from bats to camels, and which doesn’t seem to easily spread from person to person.
Both SARS and MERS coronaviruses are far deadlier than their cousin — SARS had a case fatality rate of almost 10 percent, and MERS nearly 35 percent, compared to an estimated rate of between 1 and 2 percent for Covid-19. But SARS and MERS transmit far less easily.
How does it spread?
The virus spreads fairly easily from person to person, through droplets that travel through the air when people with infections breathe, cough, or sneeze. These droplets can land on surfaces, where the virus can remain viable for some period of time (maybe between 3 and 72 hours depending on the surface type, we’re not sure yet). When you come in contact with the virus on a surface, you can pick it up and accidentally transfer it to your mouth or nose when you touch your face.
According to a WHO study of cases in China (PDF), the majority of spread of the virus has been in households among families, which suggests that more than casual exposure (just walking past someone infected) is required to catch the disease.
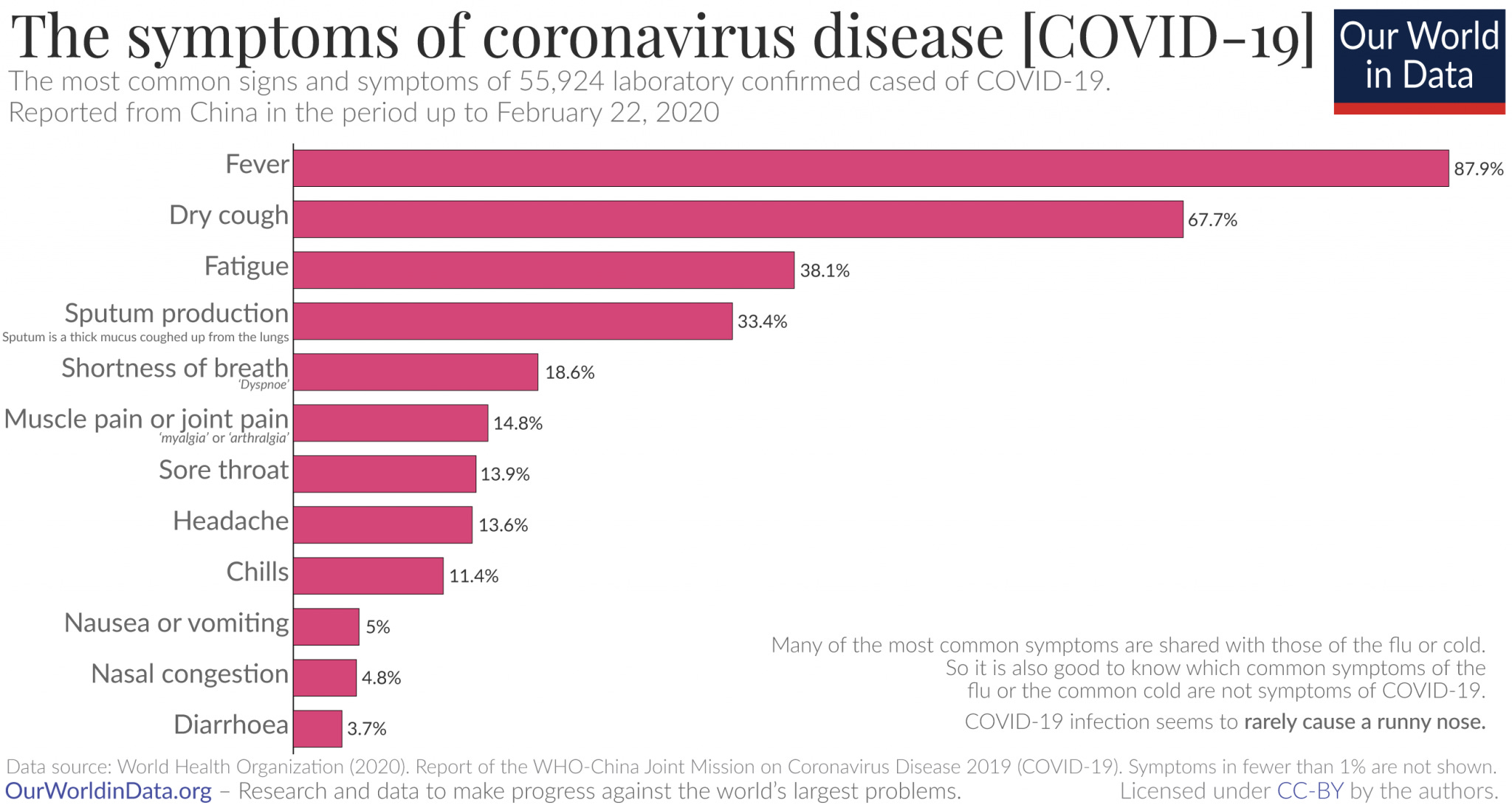
What are the symptoms?
Symptoms tend to start within 5-6 days of exposure, most frequently with a fever and dry cough. Nasal congestion and runny nose are rarely associated with this disease, according to analysis of confirmed cases in China. Symptoms generally last 2 weeks. There are conflicting reports about whether or not asymptomatic people can spread the virus, but it does seem likely that people can spread the disease even while their symptoms are very mild (and so more likely to be going to work and generally being in public).
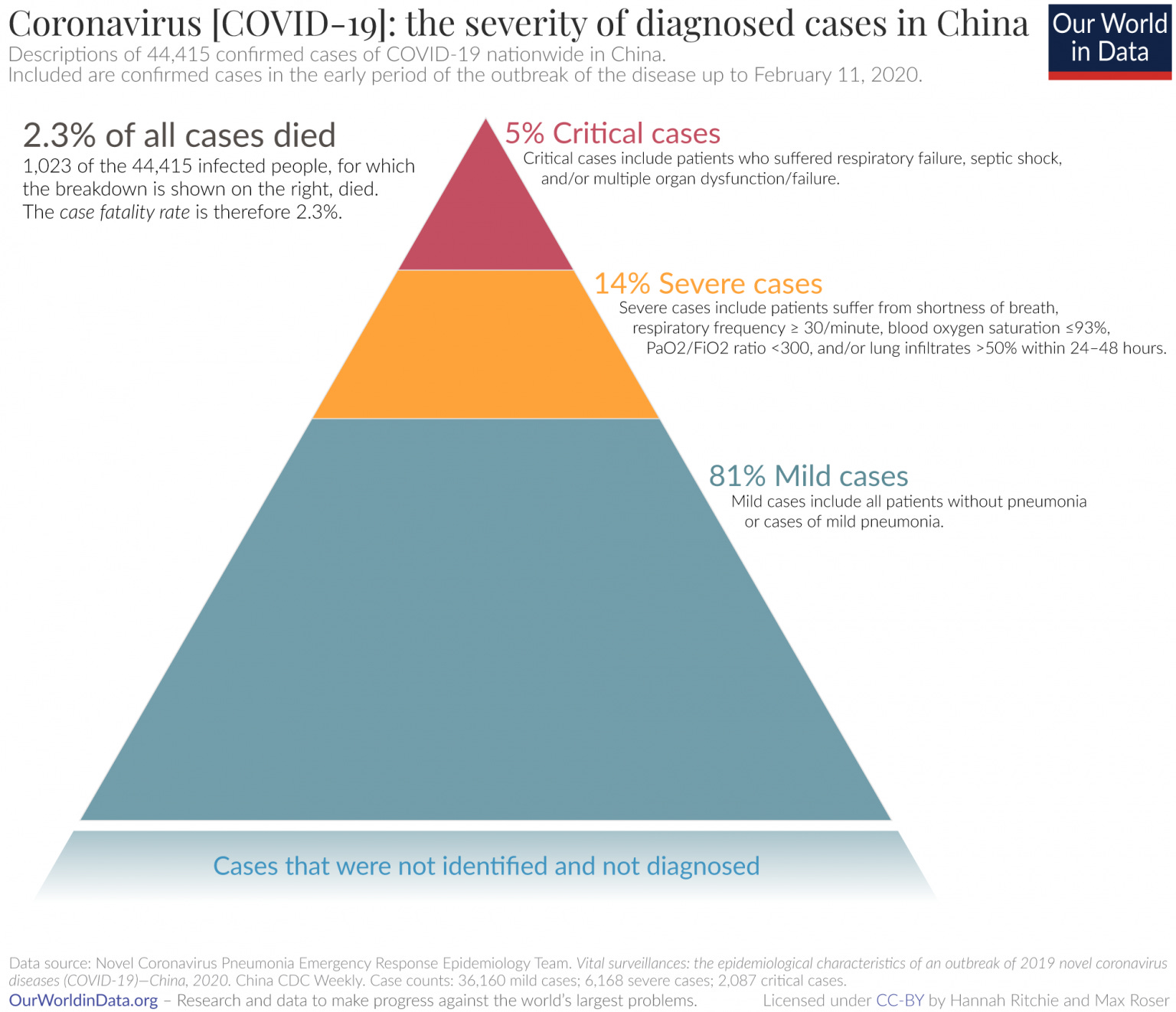
How severe is the illness?
You will have heard that most cases are mild. This is true, though even clinically mild cases can include pneumonia, which can be seriously unpleasant. Again from the largest dataset of cases we have, from China, below is the breakdown of symptom severity for confirmed cases.
Don’t focus too much on the case fatality rate (CFR). It changes over time, and is a reflection of how many cases we’re detecting, what population is being infected, and the state of the healthcare system in which people are being treated. That last note is important: outside of the fatalities is a much wider population of people who need to be hospitalized in order to survive. Hospitals in Wuhan were rapidly overwhelmed in the early stages of the outbreak there, as they have been in northern Italy, and as they are likely to be in the United States.
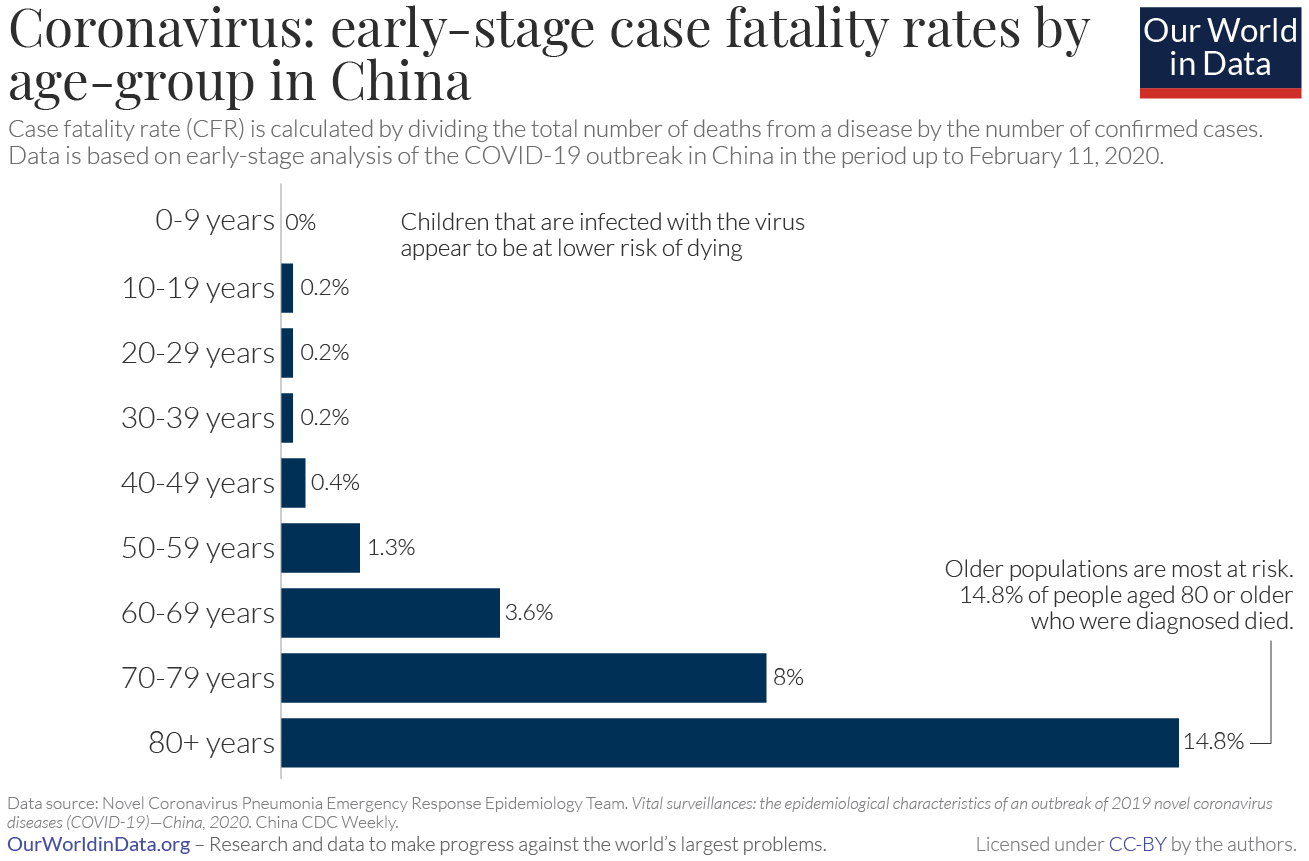
Does age matter?
Yes! Young children appear not to suffer serious symptoms, though they may be able to spread the virus to others. The danger increases rapidly in older patients. Note the uptick starts noticeably in the 40-49 age group here, though even people in their teens and twenties can become seriously ill or die (as this moving story of two young medical professionals from Wuhan illustrates). The danger is dramatically higher for patients above 60 years of age. This is why long-term care facilities and senior homes have been the stage for so many tragedies in the U.S. already.
Isn’t this just like the flu?
No. At the moment, the rate of fatalities from Covid-19 is estimated to be between 1 and 2 percent, at minimum ten times more deadly than seasonal flu. People have no natural immunity to this virus, there is no vaccine, and no specific treatment to combat the virus directly. This means not only are infections difficult to fight, they spread rapidly within communities, which overwhelms the medical system’s ability to treat people’s symptoms. We take for granted how well-protected people are today from most infectious diseases, relative to generations past. As Neil Fishman, an infectious disease specialist, told the Wall Street Journal: “what we’re seeing with Covid-19 is what influenza would look like without a vaccine.”
This has serious secondary effects — when hospital beds are full of Covid patients, there’s less capacity to treat other people for all the usual things people go to hospitals for.
How bad is it likely to get in the U.S.?
(Caution, read carefully here)
This really depends on a number of factors, including how aggressively people self-isolate, how quickly the hospital system ramps up capacity, and how quickly treatments and vaccines are developed.
//-!
I want to pause here to emphasize the uncertainty around these projections. This isn’t like forecasting the path and intensity of a hurricane, which is itself an impressive feat of science. It might be obvious to say, but hurricanes don’t change their paths in response to our forecasts (it’s not obvious to everybody). Projections of a pandemic can to some extent change its future course — especially if the projections, for lack of a scientific term here, scare the bejeezus out of people so they are more likely to comply with social distancing, testing, vaccination, and other public health measures. Or if they scare decision-makers into taking the advice of their public health experts.
!-\\
That said, a leaked projection of a two-month Covid epidemic wave presented to the American Hospital Association in late February estimated 96 million infections, 4.8 million hospital admissions, and 480,000 deaths:
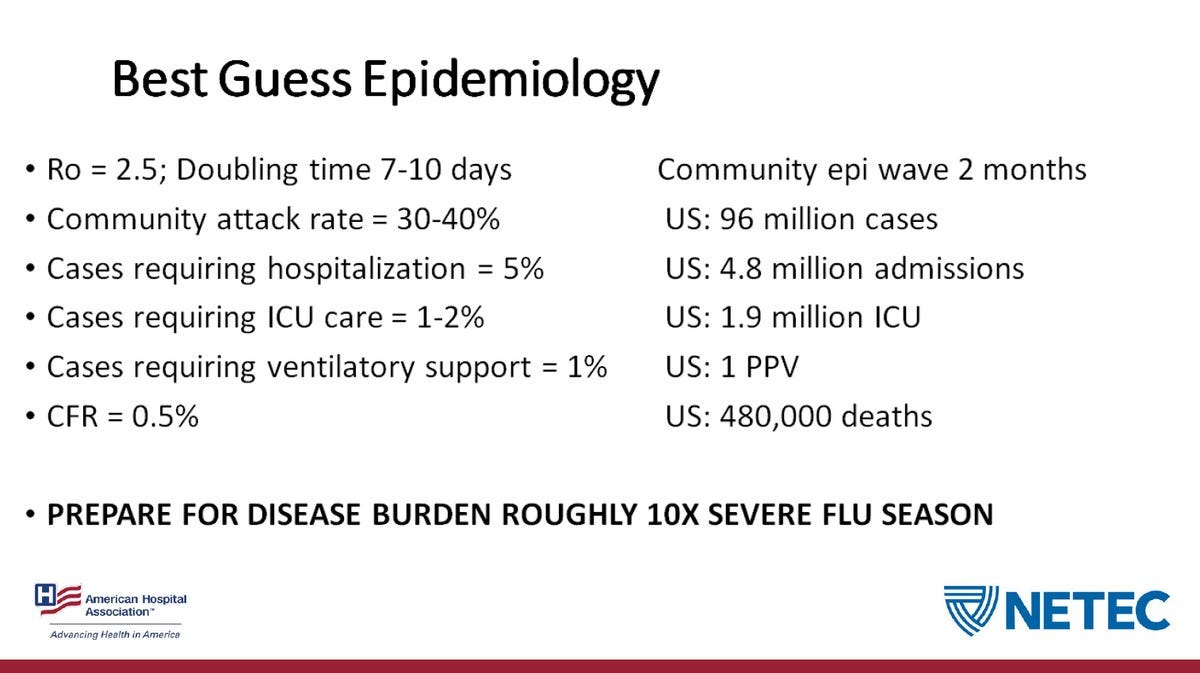
This projection is in line with modeling from the Centers for Disease Control and Prevention, which estimated between 2.4 million to 24 million hospitalizations, and between 200,000 and 1.7 million deaths.
It’s unclear to me, personally, what health interventions were built into these models. Are they based on assumptions of school closures, prohibition of public gatherings, mandated tele-work, and a massive slowdown in travel by air, rail, and bus? Or are they based on zero intervention? These are things I personally don’t know and haven’t seen specified in any reporting, and if anybody knows, I’d love to hear it.
One absolutely crucial thing you’re maybe already tired of hearing is that we have to #FlattenTheCurve, or take actions to slow the rate of infection so we can reduce the burden of the disease on the health care system. It is extremely unlikely now that the virus can be contained. But if the pandemic infects the same number of people over a longer period of time, it will claim fewer lives. Aside from hospital capacity, it is also important to slow the spread of infection because it buys us time to develop a vaccine, which is at least a year away.
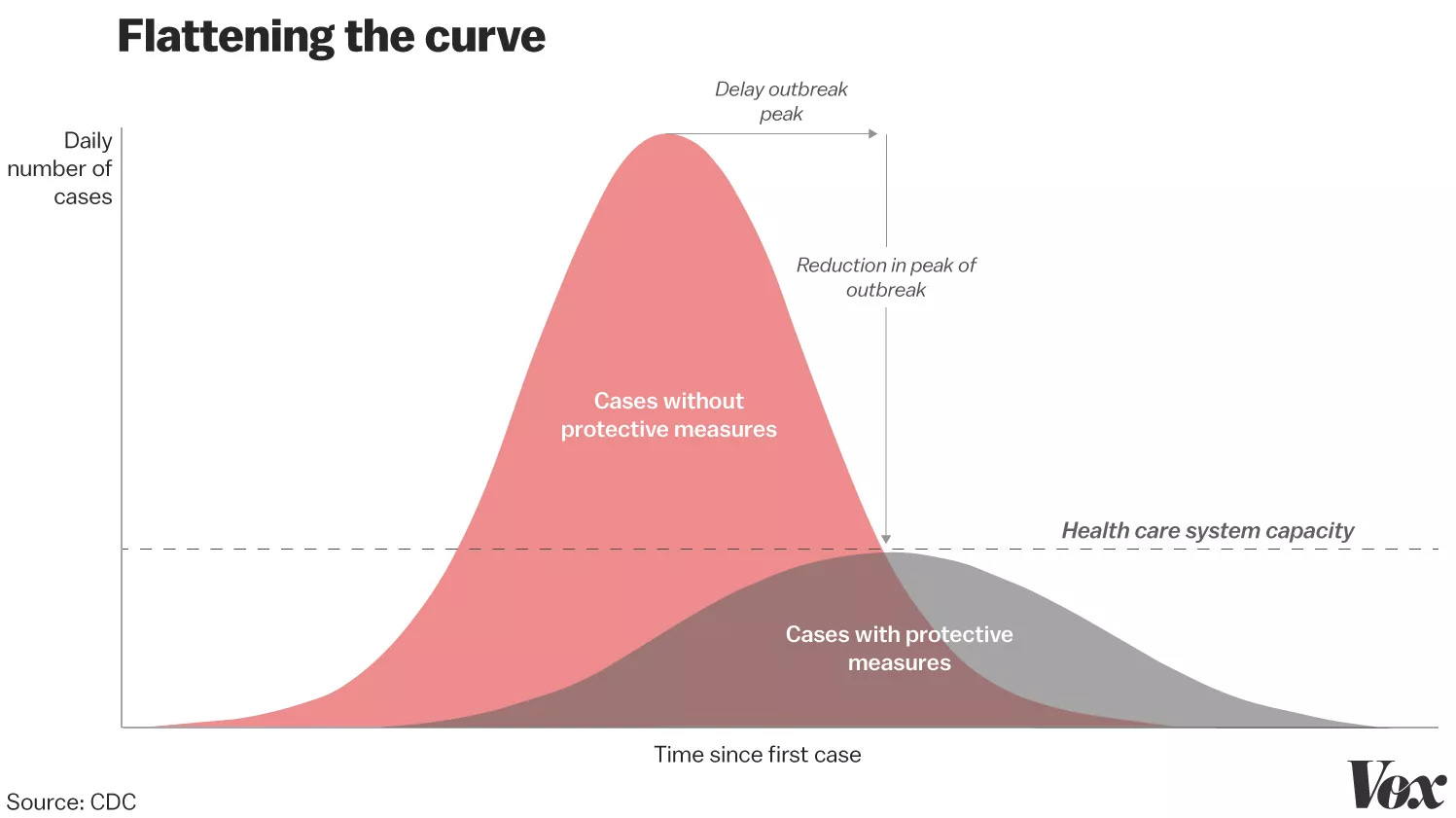
This is to say, the current wave of closures and cancellations might make it seem like things are getting worse and out of control. Exactly the opposite — it means the virus will spread more slowly than it would have if everyone had kept going about their business as usual. It’s not an exaggeration to say that when you take part in social distancing, even if you’re not sick yet, you’re fighting the pandemic and saving lives.
Why does testing matter, and what went wrong with it?
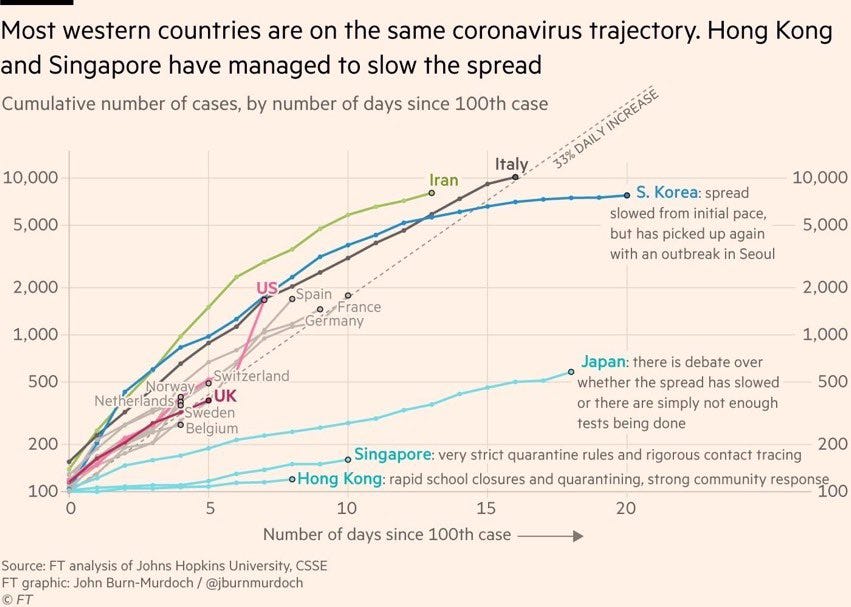
In places where the rate of infection has been slowest or where it has been slowed — Hong Kong, South Korea, Singapore, China — intensive testing to detect where the virus is in the population has been a powerful tool, so that people with infections can be isolated before they spread it to too many others. This testing is multi-layered, beginning with widespread temperature checks to detect people with fevers, rapid CT scans (in the case of China) to detect signs of infection in the lungs, and ultimately a PCR (polymerase chain reaction) test to detect the physical presence of the virus itself in a person.
If you’re having a hard time seeing where the virus is, you can either assume it’s everywhere, and shut down everything, or assume it’s only in the few places you’ve looked, and do little or nothing. The U.S. is having a very hard time seeing where the virus is, because for a complicated set of reasons (this is the best account I’ve read so far) the country has been unable to produce, distribute, and process enough testing kits. South Korea has been testing nearly 20,000 people a day to get a handle on their corner of the Covid outbreak. The U.S. has struggled to test fewer than 14,000 people total since the first cases were reported here in mid-January.
The U.S. testing bottleneck inspired some dark memes on Twitter drawing on HBO’s (incredibly good and generally relevant) Chernobyl miniseries, a scene in which a complacent engineer downplays the radiation danger following the nuclear accident because the dosimiters on site only measured 3.6 roentgen (a dose of radiation that’s “not great, not terrible”). Only, the on-site dosimeters were cheap and couldn’t measure above 3.6 roentgen. The real number was above 10,000.
By the CDC’s official count on its website — which during this rapidly developing situation currently only updates at noon, Monday through Friday and apparently not at all on weekends — there are 1,629 confirmed cases of Covid-19 in the U.S.
We can’t know the true number of current cases for certain. But Trevor Bedford, a scientist at the Fred Hutchinson Cancer Center in Seattle, whose research team sounded an early alarm that the spread of Covid in Washington State was likely much wider than PCR testing showed, estimates the true number is anywhere between 10,000 and 40,000.

How long will this last?
Likely many months. The virus may retreat during the summer, only to roar back the following the fall, like the 1918 flu pandemic. There’s possibility that it will become endemic, becoming the fifth regularly circulating human coronavirus. But in that case, it should become less deadly as people acquire natural immunity and a vaccine and treatments are developed.
But the quarantines and shutdowns will, eventually, inevitably, end. We’re not going to be cooped up in our houses forever.
// Things I’m watching for
Italy or South Korea? This may have been the week when people in the U.S. started really taking this pandemic seriously, but it’s next week and the week after when we’ll start to have a better sense of the trajectory we’re on. The conventional wisdom for a lot of folks seems to be that we’re a week or two behind Italy on the epidemic curve. The European CDC on March 12 noted that because of “the speed with which COVID-19 can cause nationally incapacitating epidemics once transmission within the community is established … in a few weeks or even days, it is likely that similar situations to those seen in China and Italy may be seen in other EU/EEA countries or the UK.” If the U.S. is going to mirror Italy’s rapid descent into a near total shutdown, the first signs of it should appear in the coming week or two.
Rumor control? I’m not especially fond of the WHO’s term “infodemic” to describe the spread of misinformation associated with public health emergencies. But the phenomenon is undoubtedly real and dangerous. Recently in New York Mayor DeBlasio took time out of a press conference to swat down online rumors that the city was about to quarantine Manhattan (it isn’t). How much of the ‘fake news’ in this environment will be honest anxiety, trolling, and how much will be intentional sabotage of the public sphere?
Unexpected consequences? Society is complexly interconnected, and shutting down circulation of people and goods is going to have weird consequences we didn’t see coming, and they will take a while to start showing up.
Will we learn how to social distance? Large gatherings are banned but how should we make everyday choices about the smaller gatherings we count on to stay sane?
What in the world is going on with… world leaders? The rapid spread of Covid-19 among Iran’s parliament and ruling elite was a sign of how widely the epidemic had spread there. So what does it mean that political elites (including possibly President Trump, who claimed he underwent testing today) are apparently coming down with it in droves?
// Further resources & what I couldn’t fit
Substack notifies me I’m running out of space in this first issue (note: use an editor), but wanted to leave you with a video of this expert panel discussion on Covid at Harvard from March 6th. The first question was something like: “Was it a mistake for us to all be here today?” Everyone laughed except for the epidemiology professor on the panel, who replied that this was probably the last public event he would attend. Harvard shut down and evicted its students from campus four days later.
Things I hope to cover starting next week
More detail on what pandemic countermeasures actually look like in Singapore, China, and South Korea.
Implications of the “Very Big” national emergency declared yesterday.
Unintended consequences of school and business closures.
More in-the-weeds frequently asked questions from friends.
Other things I’m reading and resources for keeping up to date.
// In closing
If you’ve read to the end here, thank you for joining me. Newsletters: not great, not terrible, right? Send me any questions or feedback by email. I’ll respond individually, and start next issue with a round-up. Also, of course, expect a supplemental issue if conditions warrant!
Thank you again for reading!
-R